Spine age estimation using deep learning in lateral spine radiographs and DXA VFA to predict incident fracture and mortality
Authors: Sang Wouk Cho, Namki Hong, Kyoung Min Kim, Young Han Lee, Chang Oh Kim, Hyeon Chang Kim, Yumie Rhee, Brian H. Chen, William D. Leslie, Steven R. Cummings
Journal: medRxiv
Published Date: March 28, 2025
Citation: Cho, Sang Wouk, et al. "Spine age estimation using deep learning in lateral spine radiographs and DXA VFA to predict incident fracture and mortality." medRxiv (2025): 2025-03.
Abstract:
Background: Spine age estimated from lateral spine radiographs and DXA vertebral
fracture assessments (VFAs) could be associated with fracture and mortality risk.
Methods: In the VERTE-X cohort (n=10,341, age 40 or older; derivation set) and KURE
cohort (n=3,517; age 65 or older; external test set), predicted age difference was
defined as estimated spine age minus chronological age. The primary outcome was
incident fracture. Secondary outcomes included morphologic vertebral fracture,
osteoporosis, and incident mortality.
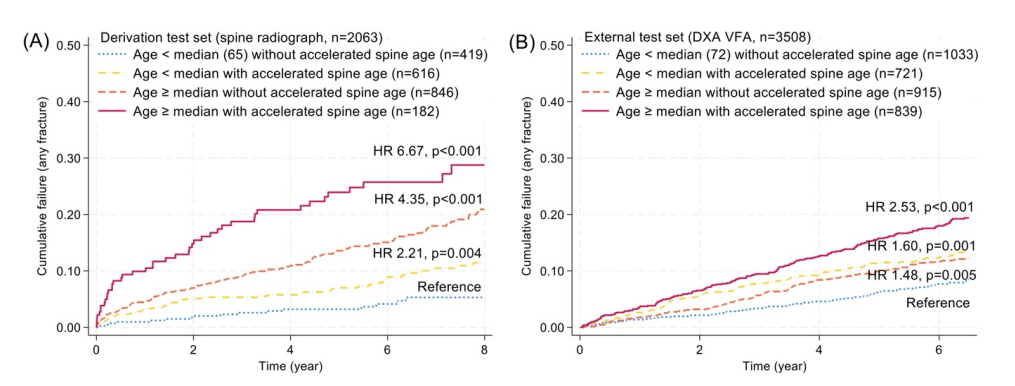
Results: Incidence of overall fracture was 20.5/1000 and 21.0/1000 person-years
(median follow-up 5.4 and 6.6 years) in VERTE-X and KURE, respectively. Spine age
discriminated prevalent vertebral fractures and osteoporosis better than chronological
age. Higher predicted age difference (PAD) was associated with greater risk of overall
(VERTE-x: adjusted HR [aHR] 1.71; KURE: aHR 1.22 per 1 standard deviation [SD]
increment), vertebral (aHR 1.55 and 1.34), and non-vertebral fractures (aHR 1.89 and
1.15, p<0.05 for all), independent of chronological age and prevalent vertebral fracture.
FRAX hip fracture probabilities based on spine age improved discrimination for
incident hip fracture over chronological age (AUROC 0.83 vs. 0.78, p=0.027). Shorter
height, lower femoral neck BMD, diabetes, vertebral fractures, and surgical prosthesis
were associated with higher predicted age difference, explaining 40% of variance. In
the external test set, higher predicted age difference was associated with greater risk
of mortality (aHR 1.31 per 1 SD increment, p=0.001), independent of covariates.
Conclusion: Spine age estimated from lateral spine radiographs and DXA VFA
enhanced fracture risk assessment and mortality prediction in adults.